Until recently, the practice of primary care medicine seemed to ignore obesity as a primary disease and focus solely upon treating the complications of obesity. Appropriate guidelines and standards for treating Diabetes, Hypertension, Hyperlipidemia, Sleep Apnea, Osteoarthritis, Coronary Artery Disease, and other complications of obesity have existed for years. However, this all began to change June 8, 2013 with the declaration by the American medical Association that obesity is a disease. This completely puts to rest the approach to obesity as solely a behavior problem. In a recent research report, the Global anti-obesity drugs market is expected to grow at a CAGR of 39.45% over the next five years. Arena Pharmaceuticals (ARNA), Orexigen (OREX) and Vivus (VVUS), investors are looking at the growing rates of obesity worldwide because the anti-obesity drugs market offers huge opportunities for investors and drug makers to profit from the paradigm shift in addressing the largest health crisis in history with pharmacotherapy.
Investor profits are premised on doctors embracing adjunctive pharmacotherapy in the treatment of overweight and obese patients. There are currently many important guidelines for the diagnosis and treatment of the obesity related conditions. These are clinical evidence-based guidelines. It is important to understand the impact that Evidence-Based Guidelines have in the healthcare practice. Evidence-based guidelines tell the physician what the recommended course of action is if the evidence in the clinic presents itself. For example, Evidence-Based Guidelines require that hemoglobin a1c be less than 7.0 to demonstrate optimal diabetes management. This is admittedly an esoteric concept, but it will ensure the success of weight loss medications. Perhaps all of them. Certainly the only unique new chemical compound, Belviq, which was developed in over a decade of research to treat obesity. These guidelines will have more impact on script growth than direct to consumer advertising, drug reps, patient requests etc. It is not a theoretically good idea. It is actually happening now. It began with a bit of a whimper a year ago when the American Heart Association, American College of Cardiology, The Obesity Society began to make evidence-based guidelines for obesity treatment. Most investors completely missed that in November 2014 the American College of endocrinology and the American Society of clinical endocrinologists issued new guidelines as to who should be considered for medication treatment for obesity and those overweight with comorbid problems (Comorbid problems means the health consequences of obesity such as diabetes and hyperlipidemia). It deserved a wow, but analysts have not yet figured out how this will change healthcare behavior. The American College of endocrinology is the governing body that the American Medical Association, the American Academy of Family Practice, American College of Physicians, and others looked to for guidance on treatment of obesity. There is no one that will come in and trump these guidelines. These are the guidelines physicians are required to follow. This is how physicians will treat obesity and overweight conditions in the United States and other countries. At the moment, the guidelines indicate who should be treated with medications. There will be additional information about the details available in January. For any non-clinician who is interested in further details I would recommend that you read Medscape Medical News from November 14, 2014 and November 21, 2014.
These guidelines have expanded to include those who qualify for medication to 116 million residents of the United States. 32 million should be considered for bariatric surgery. Dr. June Stevens of the University of North Carolina, Chapel Hill is a leading Obesity author and co-author of the original guidelines that were further published in 2013. Dr. Stevens describes the changes that occurred in November 2014 as "staggering."
Again, this is not just a good idea, these are treatments that need to be done in order for a physician to be considered as providing adequate healthcare. Insurance providers are already beginning to collect data on each covered patient's BMI. The patients are either penalized for not providing this data or rewarded for providing the data. They will provide the data. A large number of insured people are doing it right now as insurance policies are being renewed. The analyst don't know this either.
The prescription sales data, is evidencing a slow process, that may accelerate in 2015, given that in 2014, The American College of Endocrinology issued a position statement and gave a clear recommendations for using pharmacotherapy.
Recently, this advanced framework was approved by AACE and is being distributed to wide array of stakeholders who attended the Consensus Conference on Obesity for structured discussion and creation of a consensus diagnosis that is broadly actionable by primary care physicians and specialists alike:
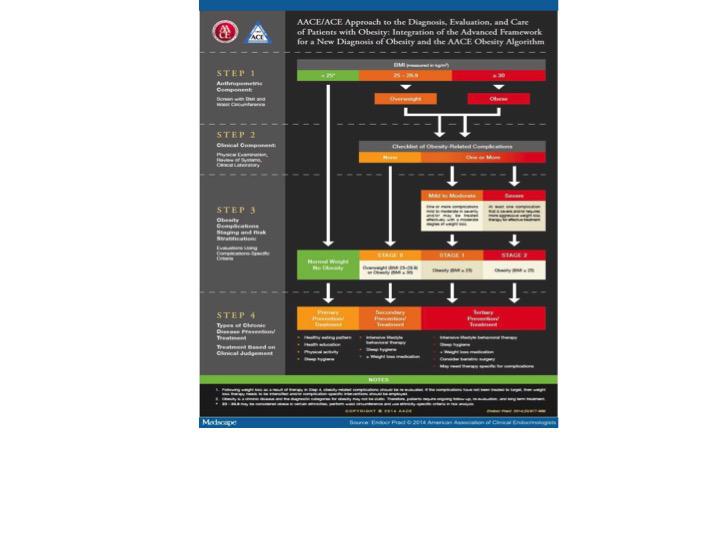
The advanced framework in the table above has been approved by AACE for a new way to diagnose and treat obesity, as a chronic disease. This framework was introduced to physicians as an 'emergent concept' for an actionable recommendation in the management of patients. AACE let physicians know it believes in taking a "complications-centric" approach to treating the disease, rather than relying heavily on body mass index (BMI). A report of the American College of Cardiology/American Heart Association task force on the new national practice guidelines and the obesity society urge doctors to focus on obesity. In its recent seventh report The Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC-8) recognized obesity as a risk factor that needs to be managed by physicians.
The end result is that physicians who practice primary care medicine will undoubtedly have their outcomes measured for weight loss treatment. Already in the medical literature and per the FDA's benchmark for approvable weight loss medicines, the goal of losing 5% of your weight at 12 weeks is becoming a standard of care marker. The doctor will find a way to make this happen if possible through combination pharmacotherapy, dieting and change in lifestyle. The three currently approved drugs Belviq, Qsymia, Contrave all have about a 50% success rate of meeting this goal at 12 weeks for those who continue on the medication. Again, it's outcomes driven. The doctor will have no interest in averaging in the responders and non-responders to determine an average weight loss number. The doctor will be interested in what medicine can safely get his patients to the weight loss goal. The next step for Big Pharma and the healthcare associations is, keep it simple. Is it safe? Is it a simple and clean drug? In my opinion, as first-line treatment, the physician would rather not have to deal with the interactions of two generic medications combined in to one pill and marketed as a name brand weight loss drug. The physician will not spend the three minutes available to discuss this topic among many that have to be accomplished that day trying to explain what a black box warning means for his patients either.
If the patient is not achieving success with first-line treatment, then consideration of a combination therapy is reasonable as second line therapy. The doctor may choose one of the pre-combined generic combos marketed as Contrave or Qsymia. The position will have approximately the same 50% success rate of achieving the optimal weight loss outcome. Alternatively, the physician may choose to write two prescriptions at the same cost as Belviq plus $15-$20 for the Phentermine coadministration and achieve an 84.2% chance of losing 5% body weight at 12 weeks. I don't believe some of the ridiculous statements that I have read on message boards that states that an insurance company will not cover two weight loss medications. I say this because this is no different than saying the insurance company will not cover two medications to treat diabetes or cancer. That statement reflects a fundamental lack of understanding of the insurance coverage and treatment process.
A convergence has started where physicians are beginning to experience the use of pharmacotherapy as an adjunct for weight loss and weight management. Most experts believe a progressive approach to obesity pharmacotherapy perhaps offers the best opportunity to finally address the obesity crisis on a mass scale. The AACE CCO developed a new diagnostic algorithm that is mapped to evidence-based risk-stratified patient subsets, and apply the AACE/ACE complications-centric obesity management algorithm. The new definition and diagnostic algorithm developed by AACE/ACE is actionable and medically meaningful, and represents a translation of the findings of the CCO task force. I believe this marks a paradigm shift because in the past, the lack of medically meaningful strategy and poor translation of accumulating scientific data regarding the pathogenesis of obesity as a chronic disease has limited the effectiveness of public health initiatives.
Bottom Line:
I believe Evidence-based guidelines will have an important impact on the use of pharmacologic agents for the treatment of obesity. This impact is imminent. It is far more important than any catalyst you have previously read about. Perhaps more important than all the catalysts you've read about combined. It will be noticeable. The physician will be under pressure to produce a positive outcome. The safest path to this outcome is Belviq as a single agent. The most effective path to this outcome (and perhaps no safety compromise) is Belviq plus Phentermine.